AI is Outperforming Human Radiologists
Medicine has always been about pattern recognition. Hippocrates described the faces of the dying. Nineteenth-century physicians sketched chest deformities in notebooks. Radiologists learned to peer at X-rays and mammograms, searching for shadows that meant life or death. Diagnosis is built on spotting patterns — and on remembering them.
But the human eye and brain have limits. Fatigue dulls them. Training biases them. Expertise sharpens some edges while blunting others. AI enters here, not as a replacement but as an unblinking partner: a pattern hunter that never tires, capable of sifting through millions of pixels and billions of data points to see what no single physician could.
Radiology has always stood at the cutting edge of medicine’s relationship with technology. From X-ray films to CT and MRI, radiologists adapted to wave after wave of innovation. But as Dr. Curtis Langlotz at Stanford University explains, nothing compares to the transformation brought by artificial intelligence.
“I remember the exact moment I realized AI would change everything,” Langlotz recalls. “I was reviewing chest X-rays late one evening when our experimental AI system flagged a subtle nodule I had missed. It wasn’t just that the AI found something I didn’t—it was the realization this technology could work alongside me, making me a better doctor.”
This is just the beginning. While the prevailing sentiment, especially among healthcare providers, is that the emerging AI-driven technologies improve what human radiologist and diagnostic experts are capable of, the actual results show that AI working on its own is more accurate, efficient and much less expensive. In some applications by a wide margin.
The Challenge of Early Detection
Few cancers illustrate the stakes more starkly than lung cancer. It remains the leading cause of cancer death worldwide, in large part because it is usually diagnosed too late. Small nodules on CT scans may or may not be malignant. Radiologists often must decide whether to dismiss, monitor, or biopsy them — and the uncertainty can cost lives.
At Google Health, Dr. Shravya Shetty and her team took on this challenge. Working with the National Cancer Institute and major medical centers, they developed an AI system that analyzes not just individual CT slices but the entire three-dimensional structure of the lungs. The system also tracks changes over time, learning the subtle textures and growth patterns invisible to the human eye.
Dr. Michael Gould, a pulmonologist at Kaiser Permanente who collaborated on the project, was astonished:
“The AI system could predict which small nodules would become cancerous with 94% accuracy. That’s better than most experienced thoracic radiologists.”
The bigger story came when the model was put into practice. At Intermountain Healthcare, thoracic surgeon Dr. Thomas Varghese oversaw deployment across the network. “We went from missing 20% of early-stage cancers to missing less than 5%,” he reported. “That translates to hundreds of lives saved each year in our system alone.”
Case Studies from the Front Lines
Across the country, AI has quietly begun reshaping diagnostic practice:
Chicago, lung cancer screening — Radiologists reviewing low-dose CT scans used an AI system that automatically ranked nodules by malignancy risk. The AI didn’t replace biopsy or follow-up imaging, but it made sure no suspicious lesion got lost in the shuffle.
New York, digital pathology suites — AI overlays helped pathologists resolve borderline prostate cancer cases. In multi-reader trials, accuracy improved, turnaround time dropped, and consistency rose.
Seeing Beyond the Human Eye
The impact is especially profound in pediatric oncology, where many doctors see only a handful of rare cancers in their entire careers. Dr. Kristen Yeom, a pediatric radiologist at Stanford, faced this challenge in diagnosing brain tumors in children.
With colleagues, she helped build an AI system that analyzed pediatric brain MRIs. At first, it simply confirmed what experts already knew. Then it began identifying features even experienced neuroradiologists had never recognized.
“The AI was picking up on subtle patterns in how water molecules moved through brain tissue,” Yeom recalled. “These were invisible to human eyes but turned out to be early indicators of tumor infiltration.”
At Boston Children’s Hospital, Dr. Tina Young Poussaint put the system into clinical use. “We reduced our diagnostic uncertainty by 60%,” she said. “For parents facing their child’s potential cancer diagnosis, that certainty is invaluable.”
The benefits extended to treatment planning. Dr. Michelle Monje, a pediatric neuro-oncologist at Stanford, used the AI to map tumor boundaries, enabling surgeons to remove malignant tissue while preserving healthy brain function. Dr. Samuel Cheshier, a pediatric neurosurgeon, described the change simply:
“AI has become our GPS for navigating the brain.”
Decoding the Genome’s Hidden Language
Patterns aren’t confined to images. Cancer also hides its signals deep within the genome. In the early 2000s, Dr. Victor Velculescu at Johns Hopkins recalled feeling overwhelmed after sequencing cancer genomes.
“We had all this genetic data, but it was like having a library in a foreign language.”
At the Broad Institute, Dr. Gad Getz built AI algorithms that could read this hidden language. His lab trained models on tens of thousands of patient genomes to distinguish driver mutations from harmless passengers. Collaborating with Dr. Shamil Sunyaev at Brigham and Women’s, they pushed prediction accuracy for harmful variants above 90%.
This marked a leap from studying individual genes to modeling entire networks of genetic interactions. What once took years of painstaking analysis now emerged in weeks, even days, giving oncologists insight into which mutations truly mattered.
CheXNet – The Stanford Breakthrough
Stanford’s AI lab, led first by Dr. Andrew Ng and later Dr. Pranav Rajpurkar, developed one of the first landmark systems: CheXNet, a deep learning model that could identify 14 different pathologies in chest X-rays with accuracy on par with expert radiologists.
The real breakthrough was not only diagnostic accuracy—it was speed and consistency. As Dr. Matthew Lungren, a radiologist and AI researcher at Stanford, explained:
“A radiologist might read 100 chest X-rays in a day and perform at 95% accuracy when fresh, but that accuracy drops with fatigue. AI never gets tired, never has a bad day, and can process thousands of images with unwavering precision.”
Radiology images are digital, high-volume, and standardized—ideal fuel for AI training. That has made radiology one of medicine’s earliest proving grounds for AI. And some say the first victim.
CHIEF – A Universal Cancer Detector in Pathology
If radiology was AI’s first proving ground, pathology may be its most ambitious. Pathologists spend hours analyzing tissue under microscopes—a process that is time-consuming and subjective. With the digitization of pathology slides, AI is transforming this field.
In 2025, researchers at Harvard Medical School introduced CHIEF (Cancer Histology Image Evaluation Foundation), trained on 44 terabytes of pathology data across millions of slides. The results were remarkable:
96% accuracy across 19 cancer types.
Ability to predict survival outcomes directly from pathology images.
Identification of genetic mutations without costly genetic testing.
Chamath Palihapitiya, a well-known venture capitalist, called it a paradigm shift, “Through more efficient evaluations, CHIEF could enable better diagnosis and treatment.” Dr. Pranav Rajpurkar, involved in its development, emphasized its robustness: CHIEF was validated on 32 datasets from 24 hospitals, overcoming one of the biggest challenges of AI—failing outside the lab where it was built.
Tissue slides hold more than meets the eye. AI can detect hidden patterns—clues to prognosis or mutations—that even the most experienced pathologists cannot see.
Large Language Models – Reasoning Beyond Images
AI’s promise extends beyond images. In 2024, a randomized clinical trial published in JAMA Network Open compared physicians’ diagnostic reasoning with and without access to a commercially available large language model (LLM).
On its own, the LLM scored a median of 92% per case—outperforming physicians.
Yet physicians paired with the LLM did not improve significantly compared to those working unaided.
The paradox was striking: the AI alone outperformed both groups of humans, but simply giving it to doctors didn’t help. Researchers suggested two reasons:
Physicians were not trained in how to interact effectively with AI.
AI needs to be integrated into workflows—for example, pointing out features that don’t fit a diagnosis, not just producing an answer.
In addition to skill level -- AI can see things that humans can’t, and AI doesn’t experience fatigue – another issue is human bias. Humans, protective of skills they’ve put years into developing, dismiss AI as unnecessary or error-prone despite evidence to the contrary. A study grounded in the Dunning–Kruger Effect found that individuals who overrate their own performance are less likely to rely on AI, hindering optimal collaboration. (Cornell study: Knowing About Knowing:
An Illusion of Human Competence Can Hinder Appropriate Reliance on AI Systems).
There are also legal and ethical concerns that shape skepticism. For instance, when AI flags an abnormality missed by a radiologist, it could increase perceived liability or “AI penalty”, so professionals may unconsciously emphasize AI's limitations to protect themselves. Medical malpractice suits may face more complex challenges with the rise of artificial intelligence, according to a study led by Brown researchers that suggested that radiologists are viewed as more culpable if they fail to find an abnormality detected by AI. (See: Use of AI complicates legal liabilities for radiologists, study finds. July 28, 2025).
AI Is More Predictive Than Humans By A Wide Margin
While humans and AI are rated roughly on par when it comes to making accurate diagnosis in terms of cancers that patients currently have, depending on the study, when it comes to predicting months or years in advance which patients will get cancer, AI has a huge advantage.
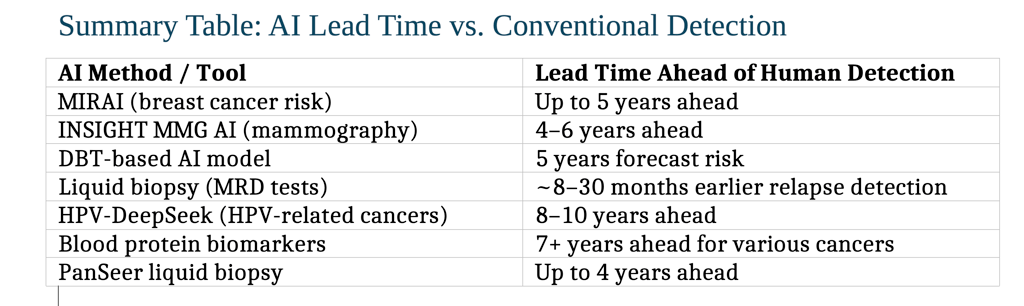
1. Mammography-Based AI (2–6 years ahead)
The MIRAI model predicts the risk of developing breast cancer up to five years in advance—demonstrating strong predictive accuracy and cross-population validation.
Massachusetts General HospitalNAMAnother study using commercial AI algorithms (INSIGHT MMG) found that AI scores were significantly higher 4–6 years before clinical detection, with AUC values climbing over time—showing meaningful lead time for early intervention.
JAMA Network News-Medical
2. Digital Breast Tomosynthesis (5-Year Forecast)
A recent preprint introduces a deep learning model using digital breast tomosynthesis (DBT) that forecasts an individual's 5-year breast cancer risk with an AUROC (Area Under the Receiver Operating Characteristic curve. It is a metric used to evaluate the overall performance of a diagnostic model, such as an AI system that analyzes ultrasound images or a risk assessment model.) of 0.80.
3. Liquid Biopsy and Circulating DNA (Months to Years ahead)
Technologies like Guardant’s Reveal, Natera’s Signatera, and others detect cancer relapse between ~8 months to over 28 months earlier than traditional imaging.
4. HPV-Related Head and Neck Cancers (Up to ~10 years ahead)
The HPV-DeepSeek test identifies HPV-associated head and neck cancers up to 8–10 years before symptoms or clinical diagnosis by detecting tumor DNA fragments via machine learning-enhanced blood testing.
5. Blood Protein Biomarkers (7+ Years ahead)
A study from the UK Biobank found that certain blood proteins correlated with a cancer diagnosis over seven years later, suggesting long-term early warning potential.
PanSeer, a noninvasive liquid biopsy, detected several cancer types in 95% of asymptomatic individuals who were later diagnosed—even up to four years before standard diagnosis.These extended lead times open new possibilities for earlier intervention, targeted preventive screening, and meaningful improvements in patient outcomes.
Patients as Pioneers – Self-Diagnosis with AI
Not all medical AI flows through hospitals. Increasingly, patients are using AI tools directly. Some stories are controversial, but others are lifesaving.
Lauren Bannon, dismissed with “acid reflux,” asked ChatGPT about her symptoms in 2025. It suggested Hashimoto’s thyroiditis, prompting further tests that revealed a neck tumor. “AI saved my life,” she said.
Marly Garnreiter had unexplained symptoms that stumped specialists until AI flagged Hodgkin lymphoma—confirmed months later.
Sam West used AI-driven statistics to identify a rare tumor variant six months before experts recognized it.
Robert Wright, after noticing a neck lump, turned to AI for guidance. It urged him to seek care, revealing throat cancer. Now cancer-free after immunotherapy, he hosts a podcast on AI in health.
These cases highlight both AI’s democratizing power and its risks. While AI can push patients toward timely care, it can also mislead, over-reassure, or spark unnecessary anxiety.
A note of caution: consumer AI tools can serve as a “second opinion” that encourages medical visits. But without clinical oversight, they can create confusion or false reassurance. Of course misdiagnosis by trained professionals is also surprisingly common.
Conclusion
Across radiology, pathology, diagnostic reasoning, and even patient self-advocacy, AI is establishing itself as a true partner in diagnosis.
In radiology, tools like CheXNet read images quickly and consistently.
In pathology, CHIEF shows the potential of universal multi-cancer detection.
In clinical reasoning, LLMs hint at enormous capability, but need workflow integration.
For patients, AI empowers—but also carries risk.
Key Implications
AI can match or surpass human radiologists in accuracy and consistency. Every day the disparity widens in favor of AI as models learn from the results of prior diagnosis.
Validation across diverse hospitals is essential before clinical adoption.
AI-human collaboration requires new workflows and training, not just access.
Patients with access to AI reach diagnoses sooner.
And there are some things only humans can do: comfort, guide, and find peace in the presence of hope and fear.
Be in touch if you'd like to talk. We can help you achieve a better result if you contact us earlier rather than later.
(843) 284-6850 (Office)
(843) 802-0183 (Mobile)
17 Executive Park Road, Office 4B
Hilton Head Island, SC 29928
(Office complex between the fire station and Stellini's Restaurant)