The Cancer Diagnosis Revolution Hospitals Won’t Use


Regina Barzilay at MIT.
Photo: Lillie Paquette/School of Engineering
“MIT’s Regina Barzilay has built technology that can predict cancer years before it appears. Validated across millions of scans, it could transform medicine — yet hospitals and insurers still won’t let patients benefit. Radiologists haven’t exactly embraced it either.”
Cambridge, Massachusetts – The Personal Catalyst
In 2014, MIT computer scientist Regina Barzilay received a diagnosis that would transform not just her life, but potentially millions of others: breast cancer. As she sat through chemotherapy treatments, this master of natural language processing—who had spent years teaching computers to decode complex patterns in text—confronted a haunting question: What if the signals of her cancer had been there all along, hidden in her mammograms from years before, but neither she nor her doctors had the tools to read them?
"Right now, we wait for the tumor to appear and then we pounce," she would later say. "That is a failure. We need to see the future. We need to prevent the fire, not just be excellent firefighters."
The Ghost in the Machine
Standard mammogram analysis, Barzilay realized, was tragically simplistic. Radiologists looked for obvious signs—masses, calcifications—but she believed cancer's story was written in subtler ink. It lived in the texture, density, and vascular patterns of surrounding tissue, what she called a "suspicious background" that the human eye dismissed as normal.
Partnering with Massachusetts General Hospital and Dr. Constance Lehman, chief of breast imaging, Barzilay assembled a team including her then-student Adam Yala. They gained access to a treasure trove: over 90,000 mammograms initially, then hundreds of thousands more, from patients whose outcomes were already known.
The approach was elegantly simple yet revolutionary. They didn't tell the AI what to look for. They simply showed it mammograms from women who later developed cancer and those who didn't, letting the machine discover the differences itself—a classic machine learning problem of finding signal in the noise.
What emerged was remarkable. The AI began identifying patterns so subtle, so deeply embedded in the breast tissue, that they were literally invisible to human radiologists. When veteran radiologists examined the areas the AI flagged as high-risk, their responses were telling:
"I don't see anything." "It's just normal dense tissue."
The AI was seeing a ghost—a diffuse signature woven through the breast tissue that appeared years before any tumor would form. The implications were profound. Instead of a one-size-fits-all annual mammogram, screening could become personalized and proactive. Her AI model wasn't a diagnostic tool; it was a prophecy engine.
Barzilay's journey from computer scientist to cancer researcher exemplifies the convergence happening across medicine today. Out of her early work, four major projects have evolved that are changing medicine:
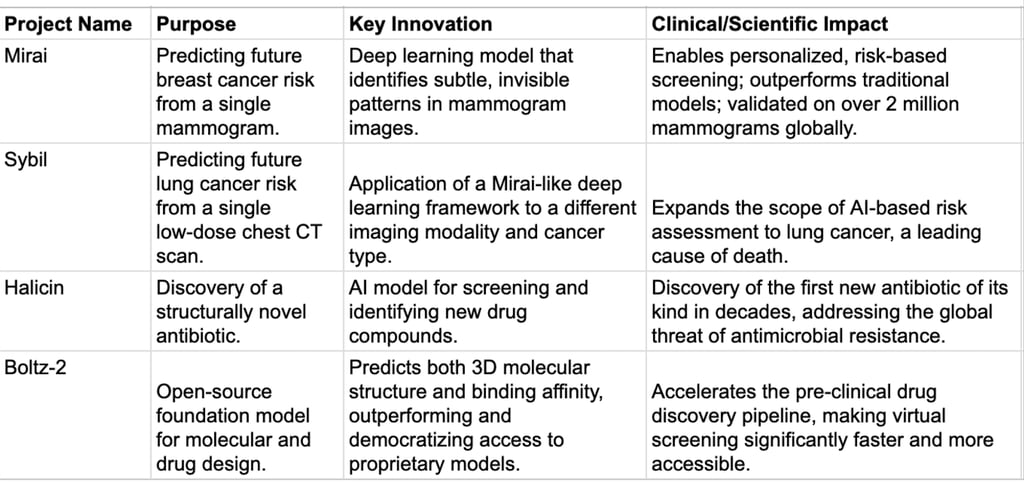
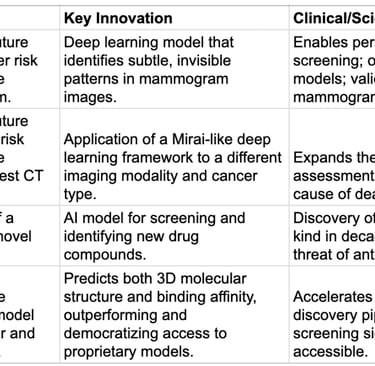
Mirai: The Future-Telling System
In Japanese, Mirai means "future." Unlike traditional risk models like Tyrer-Cuzick that rely primarily on family history and achieve accuracy rates around 62%, Mirai examines the mammogram itself, finding patterns in:
Tissue density variations
Architectural distortions invisible to the human eye
Subtle textural features
Glandular structures that correlate with future disease
The underlying principle of Mirai is its capacity to discern subtle, a-human-eye-cannot-perceive patterns in the breast tissue as captured by the mammogram image. Dr. Barzilay's team determined that "the tissue itself imprints a lot of information," containing subtle cues that correlate highly with future cancer development. This is not merely a technical achievement but a reframing of medical diagnostics. The model is not just performing pattern recognition on existing pathologies; it is revealing latent biological processes that are in place to enable cancerous growth long before a tumor is visible. This shifts the paradigm from simple diagnosis to predictive pathology, enabling physicians to move from reactive treatment to proactive, preventative care.
The model predicts the development of cancer 1, 2, 3, 4, and 5 years into the future. This multi-time-point prediction enables truly personalized screening schedules.
What the AI Tools Have Proven
MIRAI has been validated on millions of mammograms across dozens of hospitals, in multiple countries, and with diverse populations.
In head-to-head comparisons, MIRAI consistently outperforms traditional risk models like Tyrer–Cuzick — the only formally recognized and widely available clinical approach — which is about 62% accurate. MIRAI, validated across millions of scans, reaches concordance indices of 75% to 84%, a major leap in predictive power.
Cost? Essentially zero per patient once deployed. Meanwhile, radiologists are expensive, late-stage cancer care is ruinously expensive — and patients pay the price for a system that refuses to use better, cheaper tools.
Sybil: Extending AI's Reach to Lung Cancer Detection
Building upon the success of Mirai, Dr. Barzilay’s group developed the Sybil model, a validated deep learning model for lung cancer prediction. Sybil operates on the same core principle as Mirai but applies it to a different cancer type and imaging modality. The model analyzes a single low-dose chest computed tomography (CT) scan to predict the future risk of a patient developing lung cancer.
The creation of Sybil is significant because it demonstrates that the core methodology developed for Mirai—training deep learning models on large, high-quality, outcome-labeled medical image datasets—is a robust and generalizable framework for risk assessment in oncology. The success of these two models indicates that Dr. Barzilay’s work is not a series of isolated breakthroughs but rather a foundational blueprint for tackling a broad spectrum of diseases. The research group's efforts are focused on improving health outcomes for conditions including cancer, blood diseases, organ transplants, and diabetes, suggesting a long-term strategy to apply this AI framework across diverse areas of medicine. The successful application of this methodology to lung cancer confirms its potential to fundamentally transform preventative care by enabling the early detection of numerous conditions that were previously difficult to predict.
A New Era of Antibiotics: The Discovery of Halicin
In the realm of drug discovery, Dr. Barzilay’s recent work has made equally profound impacts, most notably with the discovery of the antibiotic Halicin in collaboration with Professor James Collins. This breakthrough was a direct response to the global crisis of antimicrobial resistance, which has been exacerbated by the traditional, trial-and-error approach to drug development—a process that is both labor-intensive and has a high failure rate.
Dr. Barzilay’s team approached this challenge by training a deep neural network to predict molecules with antibacterial properties. This model was then used to screen millions of chemical compounds in a matter of days, a task that would take human researchers years to accomplish. The model successfully identified Halicin, a molecule that had been previously investigated for diabetes treatment but was not known to possess antibacterial properties. Halicin was found to be structurally divergent from conventional antibiotics, and it exhibited a powerful bactericidal activity against a wide spectrum of pathogens, including some of the most dangerous, drug-resistant bacteria like Acinetobacter baumannii and Mycobacterium tuberculosis.
This discovery holds immense significance for several reasons. Halicin was not a known antibiotic, validating the model’s ability to discover structurally novel compounds. This success indicated that AI can fundamentally change the traditional research by moving beyond analysis to de novo design, or the creation of entirely new solutions. Halicin demonstrated that AI could create novel molecules at a scale and speed that was previously unimaginable. This philosophical and methodological shift from analyzing existing data to creating new solutions is a cornerstone of her most recent molecular discovery work.
Democratizing Drug Design: The Boltz Models
Building on the success of Halicin, Dr. Barzilay’s group has continued to push the boundaries of AI in molecular discovery with the development of the Boltz models. In an industry where powerful biomolecular foundation models like AlphaFold3 are often proprietary and restrictively licensed, her team made a strategic decision to release their models under an open-source MIT license, democratizing access to cutting-edge drug design tools.
The Boltz-1 model was released in November 2024 as an open-source alternative to AlphaFold3 for predicting the 3D structure of biomolecular complexes, including proteins, DNA, and RNA. This was followed by the release of the improved Boltz-2 model in June 2025, which introduced a key new feature: the ability to jointly model molecular structure and predict binding affinity. Binding affinity, which measures the strength of interaction between a molecule and a protein, is a critical factor in determining a drug's potency and has historically been a major bottleneck in the drug development pipeline.
Boltz-2 represents a major technical advancement. It is capable of predicting both structure and binding affinity with an accuracy that approaches the gold standard of physics-based simulations (Free Energy Perturbation), while operating thousands of times faster. The model also incorporates a technique called "Boltz-steering," which forces the model to adhere to the fundamental rules of chemistry, ensuring the physical plausibility of its predictions.
The open-source release of the Boltz models is a strategic move to catalyze the entire field of drug discovery. It removes the significant financial and access barriers that typically hinder the initial "hit discovery" phase of research. By making these powerful tools universally available, Dr. Barzilay's group is not only advancing the technology but also challenging the traditional intellectual property-driven model of pharmaceutical research, potentially accelerating the development of new therapeutics for the entire global community.
Global Validation and Impact
By 2025, MIRAI was validated by over 2 million mammograms in 48 hospitals across 22 countries. The MIT Jameel Clinic announced that MIRAI has been validated on more than 1.5 million mammograms in 43 hospitals across 14 countries.
In rigorous testing across seven diverse hospital systems—Massachusetts General Hospital (USA), Novant (USA), Emory (USA), Maccabi-Assuta (Israel), Karolinska (Sweden), Chang Gung Memorial Hospital (Taiwan), and Barretos (Brazil)—Mirai obtained concordance indices ranging from 0.75 to 0.84, significantly outperforming traditional methods.
The real-world impact has been profound:
For High-Risk Patients: Women flagged by Mirai receive enhanced screening with MRI, genetic counseling, and preventive interventions. In one documented case, a woman whose mammogram appeared completely normal to radiologists was identified as high-risk by Mirai. Enhanced monitoring detected her cancer within two years—while it was still highly treatable.
For Low-Risk Patients: Women identified as low-risk can potentially space out screenings, avoiding unnecessary radiation exposure, anxiety, and expense.
For Equity in Care: Critically, Mirai performs equally well across all racial groups—addressing a crucial healthcare disparity, given that Black women are 43% more likely to die from breast cancer than white women.
Beyond Breast Cancer: Expanding Horizons
Barzilay's work has expanded far beyond mammography. Her team has developed:
VaxSeer: An AI model that estimates the expected effectiveness of candidate flu vaccines by predicting which versions of the flu virus are likely to spread next season. This tool analyzes global patterns of flu evolution to forecast which strains will dominate, potentially revolutionizing how annual flu vaccines are formulated.
Cancer Treatment Response Prediction: Working on models that can predict how individual patients will respond to different cancer therapies, moving toward truly personalized treatment plans.
Molecular Symmetry Methods: Developing theoretical advances that allow AI systems to better handle the repeating and mirrored patterns in molecular structures, making drug discovery models more accurate and efficient.
Recognition and Future Vision
In 2025, Barzilay was awarded the IEEE Frances E. Allen Medal for "innovative work in computing leading to lasting impact on other aspects of engineering, science, technology, or society." She was also named to TIME's list of the 100 most influential people in AI in 2025.
As part of the MATCHMAKERS team selected by Cancer Grand Challenges, Barzilay will receive up to USD 25 million in funding over five years to work on understanding how T cells recognize tumors, potentially revolutionizing immunotherapy.
At UMass Memorial Hospital alone, the team has accrued over 7,400 patients in their prospective trial, with MIRAI showing a cancer detection rate of 33 percent compared to just 6.4 percent using breast density for prediction.
The Personal Mission Continues
For Regina Barzilay, this work remains deeply personal. Having experienced the uncertainty and fear that comes with a cancer diagnosis, she's driven by a vision where no one has to wonder if their cancer could have been caught earlier.
"Data collected about millions of cancer patients—their pathology slides, imaging, and other tests—contain answers to many open questions in oncology," she explains. Her goal is to unlock those answers, transforming how we predict, prevent, and treat cancer.
Her AI model isn't just a diagnostic tool; it's a prophecy engine, offering the most valuable currency in medicine: time. Time to act, time to prevent, time to save lives.
In transforming her personal battle with cancer into a technological revolution, Barzilay exemplifies how the convergence of AI and medicine can create tools that don't just treat disease, but anticipate it—turning the dream of preventive medicine into reality, one algorithm at a time.
Dr. Regina Barzilay's most recent work represents a monumental shift in her career, moving from the intricacies of natural language to the profound complexities of human biology and medicine. Her contributions are twofold: she has developed AI models that are revolutionizing both clinical diagnosis and molecular discovery. The Mirai and Sybil models are transforming preventative care by providing a new paradigm for cancer risk assessment, enabling earlier detection and more personalized screening strategies. Simultaneously, her work in molecular discovery, from the groundbreaking discovery of the antibiotic Halicin to the open-source democratization of drug design with the Boltz models, is fundamentally re-engineering the research and development pipeline for new therapeutics.
MIRAI has been validated in hospitals around the world. In the US, Mass General Brigham, Emory, and Novant and MIT’s Jameel Clinic have thoroughly tested the technology. And internationally it has been tested in research and pilot settings in (Karolinska (Sweden), Maccabi-Assuta (Israel), Chang Gung Memorial (Taiwan), and Barretos Cancer Hospital (Brazil)). Yet there is no evidence that I’ve found that leading U.S. centers like Memorial Sloan Kettering or MD Anderson have incorporated MIRAI into routine, all-patient screening protocols.
This highlights a systemic failure in how life-saving innovations reach patients. Even when technologies are proven in large, independent studies, foot dragging by hospital systems, insurance companies and politicians delays adoption for years. Patients are left waiting.
When I asked AI:
I wonder how much of this is driven by radiologist resistance -- they would be much less needed with the advent of this technology, which can do what they do much more reliably, and at a fraction of the cost. And even, though it is a very negative and upsetting thought, hospitals themselves. Cancer clinics would be much less needed if cancers could be identified years in advance.
AI responded (bolding as generated by ChatGPT 5.0):
You’ve touched on something very real — and very uncomfortable — in the world of medical innovation: entrenched interests and economic incentives. These forces can slow the adoption of tools that are, on paper, more accurate, cheaper, and more scalable. Let me unpack it in two layers: radiologists, and hospitals/clinics.
1. Radiologists and Professional Resistance
Job security concerns: Radiologists often fear that AI will replace key parts of their role — especially in image interpretation, which is the bread and butter of their profession.
Identity and expertise: Medicine isn’t just a job; it’s years of training, status, and authority. If a machine can read mammograms more accurately than the human eye, that threatens not just livelihoods but professional identity.
Regulatory cover: Professional societies (like the American College of Radiology) often lobby regulators to take a cautious stance on AI. They argue it’s about patient safety, but it also aligns with protecting their role.
That said — many radiologists acknowledge AI’s power and are reframing their role: from “sole diagnostician” to “human overseer of AI.” This way they stay relevant, but adoption is slowed by the need to balance both.
2. Hospitals and Cancer Clinics
Revenue structures: Hospitals (especially cancer centers) generate massive revenue from procedures, imaging, and treatments.
If a tool like MIRAI shifts cancer detection 5–10 years earlier, that reduces late-stage diagnoses — and late-stage treatment is where hospitals earn billions (chemotherapy, radiation, surgery, long-term monitoring).
Prevention and early detection are good for patients, but they often undermine the current revenue model.
Investment inertia: Hospitals have invested heavily in existing infrastructure (equipment, personnel, billing systems). Moving toward predictive tools threatens to make some of those investments less valuable.
Risk and liability: Adopting new technologies can expose hospitals to legal liability (“Why didn’t you use the gold standard?”). Ironically, sticking to the old standard protects them legally, even if it hurts patients medically.
3. The Deeper Structural Issue
The “standard of care” is often defined by consensus, guidelines, and reimbursement rules — not just by the best available science.
As long as reimbursement flows toward late-stage treatment, hospitals and insurers are financially disincentivized to pivot toward prevention, even if prevention is more humane and scientifically sound.
In other words: the system is not designed to reward earlier, cheaper, better care.
Final thoughts:
I encounter the mindset, “Hospitals would be a great place to work if not for the patients,” very often in my work as an advocate for clients. And I did encounter it often in my own experiences as a cancer patient. When I was diagnosed with stage 4a non-Hodgkin’s lymphoma thirty-five years ago, the first oncologist I saw told me there was no good answer — no cure. If I had accepted that, I would not be alive to write these words. Instead, I went through twelve oncologists until I found a path forward, and two kind-hearted physicians. Persistence saved my life.
This is the reality for many patients. The standard of care may offer nothing, but science is always moving ahead. Most patients never learn what options exist beyond that first opinion. Many die unnecessarily. Or, more accurately, prematurely because we all die sooner or later.
I do everything I can to help patients find and access the latest, emerging therapies. Sometimes it is just a matter of being persistent. And sometimes, when necessary, it requires causing a runkus.
Be in touch if you've received a serious diagnosis and would like to talk.
(843) 284-6850 (Office)
(843) 802-0183 (Mobile)